Finasteride is best known in hair loss medicine as a treatment for male androgenetic alopecia. At a lower dose, it is used to reduce scalp dihydrotestosterone, or DHT, which plays a role in pattern hair loss. At a higher dose, finasteride is also used for benign prostate enlargement.
Because finasteride affects androgen metabolism, researchers have also studied whether it changes the risk of prostate cancer. The answer is not as simple as “it prevents cancer” or “it causes cancer”. The long term evidence suggests a more careful conclusion.
Finasteride appears to reduce the diagnosis of lower grade prostate cancer, but early studies raised concern about a higher proportion of high grade cancers. Longer follow up has helped clarify this concern, although it has not removed every uncertainty.
Why finasteride was studied for prostate cancer
Finasteride blocks the type 2 form of 5 alpha reductase, an enzyme that converts testosterone into DHT. DHT is important in prostate growth and also contributes to androgenetic hair loss.
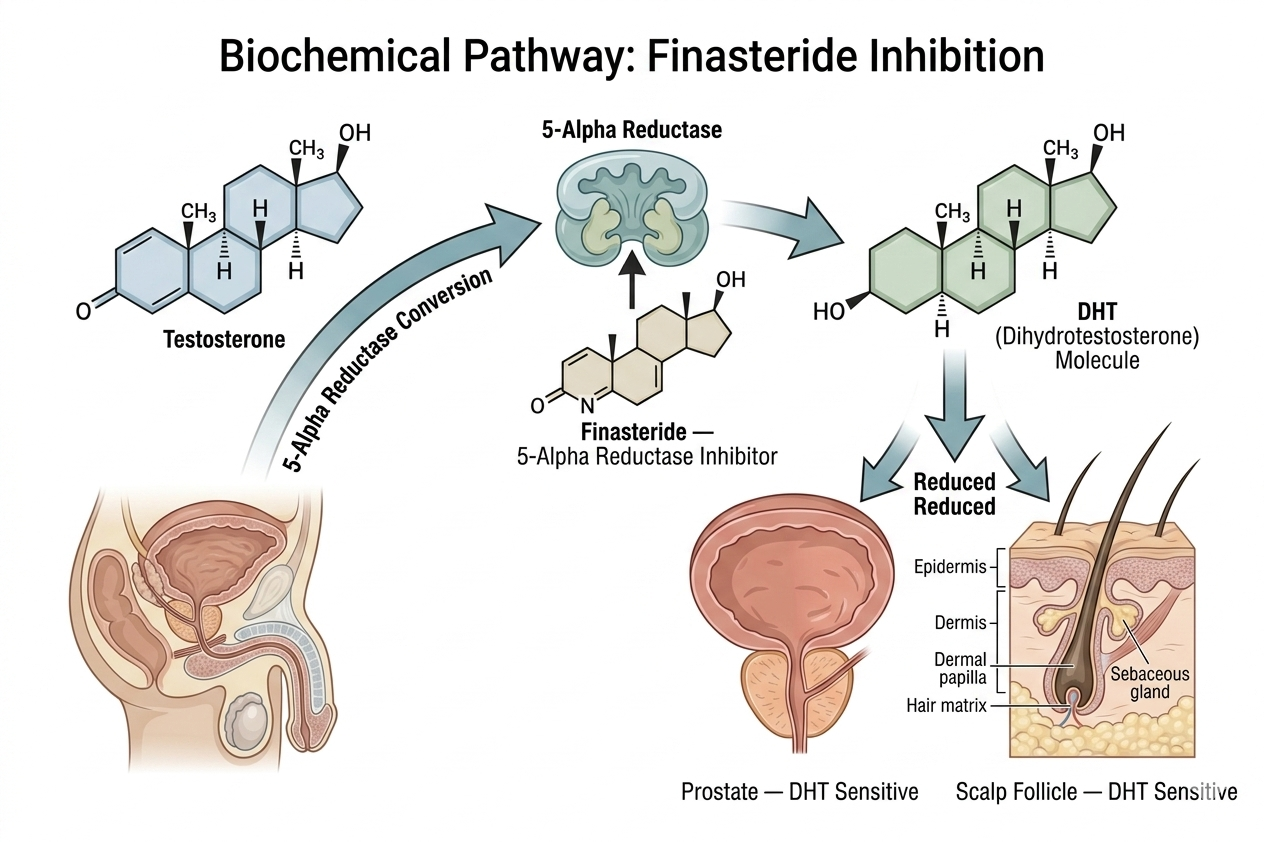
Since prostate tissue is sensitive to androgens, researchers asked whether lowering DHT could reduce prostate cancer risk. This led to one of the most important studies in this area, the Prostate Cancer Prevention Trial, often called the PCPT.
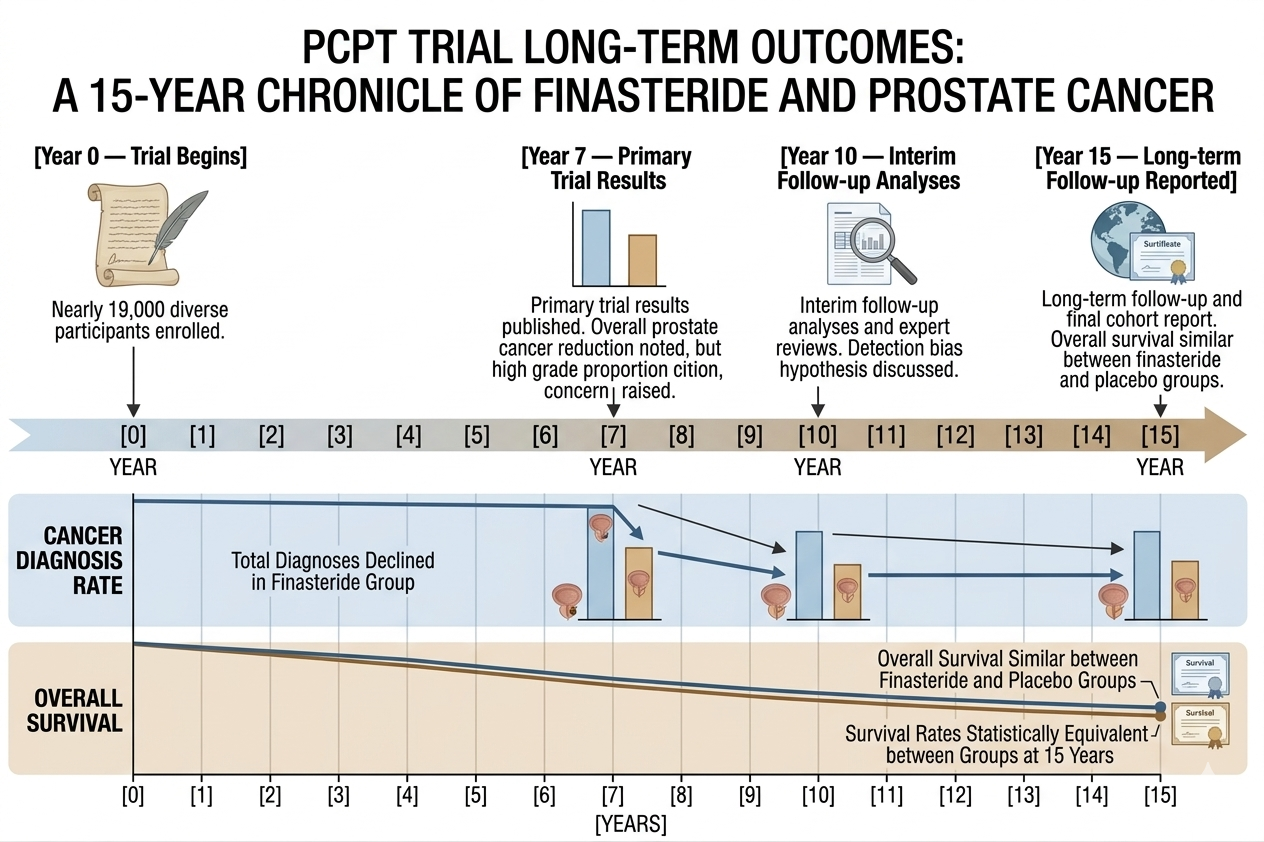
The PCPT enrolled nearly 19,000 men aged 55 and older who did not have evidence of prostate cancer at the start of the trial. Participants were randomly assigned to take finasteride 5 mg daily or placebo for seven years. The dose used in this prostate cancer prevention trial was the prostate dose, not the usual 1 mg dose used for male hair loss.
What the main trial found
The original PCPT results showed that men taking finasteride were less likely to be diagnosed with prostate cancer overall. The reduction was mainly in lower grade prostate cancers.
This was an important finding, but it came with a concern. A higher proportion of detected cancers in the finasteride group were high grade cancers. High grade prostate cancers are usually more clinically serious, so this finding led to understandable caution.
At first glance, this raised a difficult question. Was finasteride reducing harmless or slow growing cancers while increasing more aggressive cancers? Or was it changing the way cancers were detected?
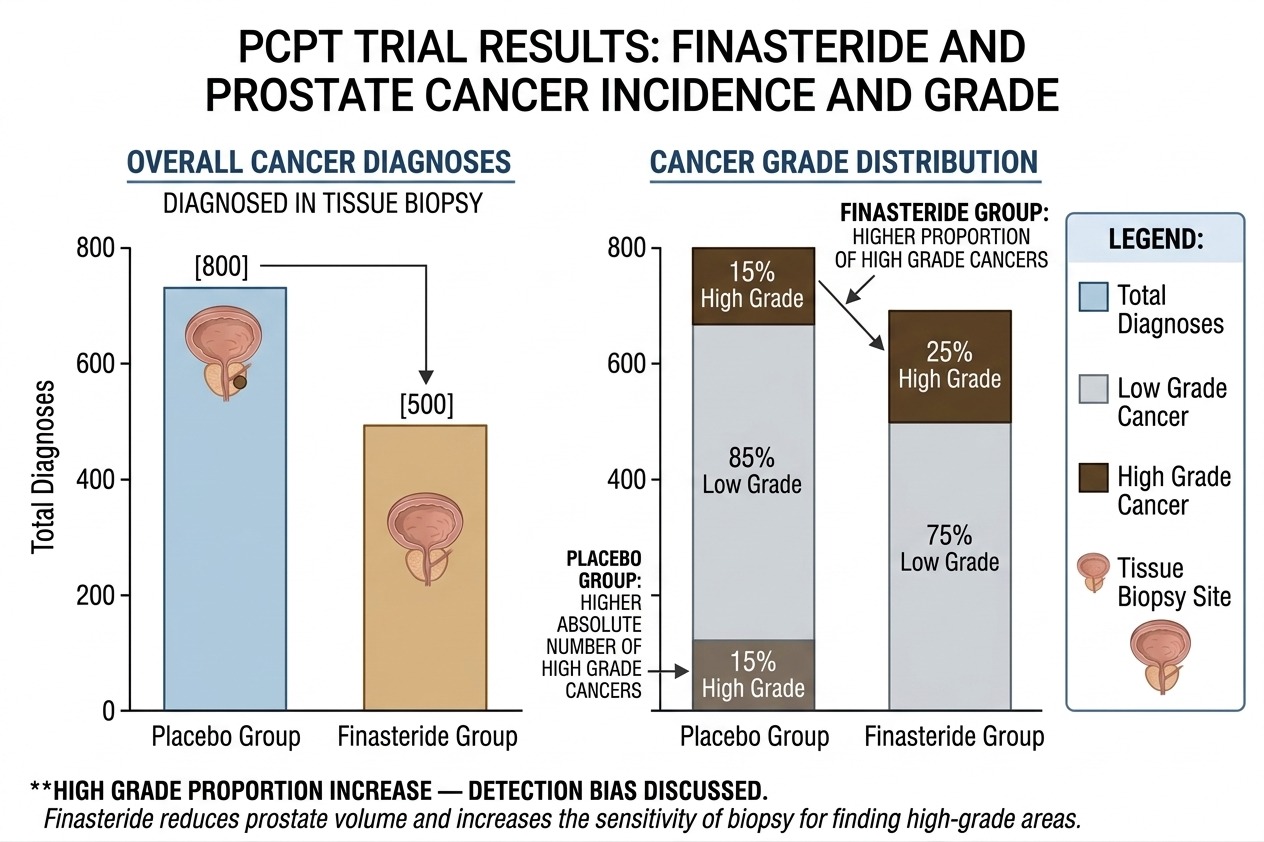
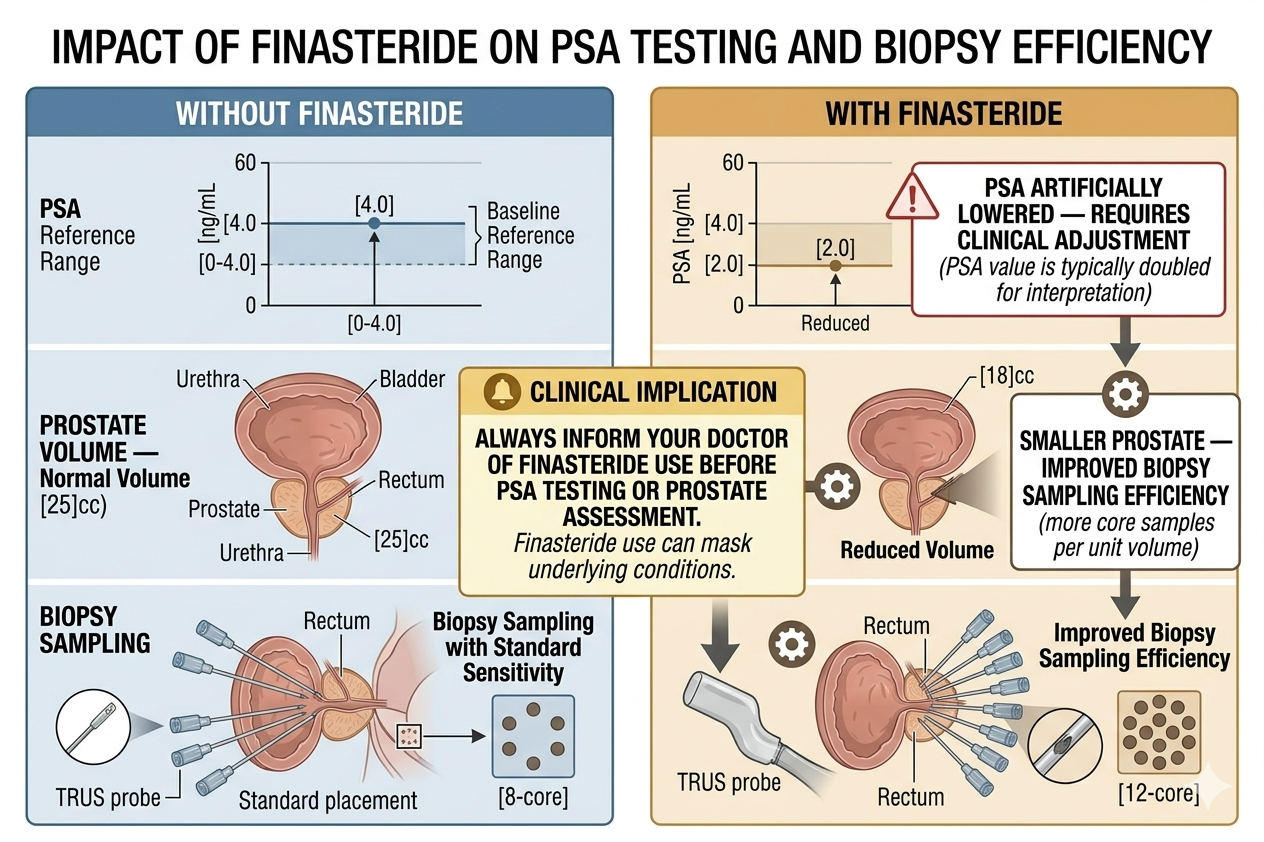
Later analyses suggested that detection effects probably played an important role. Finasteride shrinks the prostate, which can make biopsy sampling more efficient. It also changes prostate specific antigen, known as PSA, which affects screening interpretation. In a smaller prostate, a biopsy may be more likely to find an existing high grade cancer that might otherwise have been missed. The US National Cancer Institute notes that subsequent PCPT analyses suggested the apparent increase in high grade cancers was at least partly due to improved detection.
What long term follow up showed
Longer follow up was important because the early concern was not just about cancer detection. The real question was whether men taking finasteride were more likely to die from prostate cancer or have worse survival.
The long term PCPT follow up found that finasteride continued to be associated with fewer prostate cancer diagnoses, especially lower grade cancers. Although high grade cancers had been detected more often in the finasteride group, overall survival at 15 years was similar between men who took finasteride and men who took placebo.
This matters. If finasteride truly caused a major increase in lethal prostate cancers, researchers would expect to see a survival disadvantage over long follow up. That was not seen in the reported long term analysis.
Still, similar overall survival does not mean finasteride should be used routinely to prevent prostate cancer. It means the early fear of a clear increase in prostate cancer deaths was not supported by the long term survival data.
Does finasteride prevent prostate cancer?
Finasteride reduced the number of prostate cancers diagnosed in the PCPT, especially lower grade cancers. But prevention is a loaded word.
Many lower grade prostate cancers grow slowly and may never cause symptoms during a person’s lifetime. Reducing diagnosis of these cancers may lower overdiagnosis and overtreatment, but it may not always translate into a clear survival benefit.
So, a medically cautious way to say it is this: finasteride can reduce the detection of lower grade prostate cancer in older men studied under trial conditions, but it is not usually prescribed simply as a prostate cancer prevention medicine.
For men taking finasteride for hair loss, this evidence should not be interpreted as a reason to start treatment for cancer prevention. Hair loss treatment has a different goal, a different dose, and usually a different patient group.
Does finasteride increase the risk of aggressive prostate cancer?
The most balanced answer is that the trial found more high grade cancers in the finasteride group, but later analyses and long term follow up suggest this may have been influenced by detection bias rather than a true increase in dangerous cancers.
This distinction is important.
Finasteride lowers prostate volume. A smaller prostate can make cancer easier to sample during biopsy. Finasteride also lowers PSA levels, which means PSA results need careful interpretation. If PSA is not adjusted correctly, cancer assessment can become misleading.
The long term survival findings are reassuring, but not a reason to dismiss the issue completely. Any man taking finasteride should make sure his doctor knows about it when interpreting PSA tests.
What this means for PSA testing
Finasteride can lower PSA levels. PSA is a blood marker used in prostate assessment, although it is not a perfect cancer test.
In men taking finasteride, a PSA result may look lower than it would otherwise be. Doctors often account for this when interpreting the result, especially after a man has been taking finasteride for several months. The exact interpretation depends on the clinical situation, duration of use, prostate symptoms, age, and baseline risk.
This is one of the most practical points for patients. If you are taking finasteride, do not hide it from your GP, urologist, dermatologist, or hair loss clinician. It can affect how prostate screening results are understood.
Is the hair loss dose relevant to prostate cancer studies?
Most prostate cancer prevention evidence comes from finasteride 5 mg, the dose used for benign prostate enlargement. The common oral dose for male pattern hair loss is 1 mg.
Both doses reduce DHT, but they are used in different populations and for different reasons. The PCPT studied older men, aged 55 and above, not younger men taking finasteride for early androgenetic alopecia.
For a man using 1 mg finasteride for hair loss, the prostate cancer data are still useful background information. They show that finasteride can affect prostate biology and PSA interpretation. But they do not prove that taking 1 mg for hair loss provides meaningful prostate cancer prevention.
What European patients should know
In Europe, finasteride medicines are authorised for different uses depending on dose and formulation. Finasteride 1 mg tablets and some topical spray products are used for androgenetic alopecia, while finasteride 5 mg tablets are used for benign prostate enlargement. The European Medicines Agency describes finasteride as reducing DHT by inhibiting 5 alpha reductase, which is relevant to both hair loss and prostate enlargement.
European patients should also be aware that safety reviews of finasteride are not limited to prostate cancer questions. In 2025, European regulators confirmed suicidal ideation as a side effect of finasteride tablets, with frequency unknown from available data. EMA advised that patients using 1 mg oral finasteride for hair loss should stop treatment and seek medical advice if they experience depressed mood, depression, or suicidal thoughts.
This does not mean every patient will experience mood related side effects. It means the risk should be discussed openly, especially when finasteride is used for a non life threatening condition such as hair loss.
Should men with prostate cancer risk avoid finasteride?
Not always. But they should not self medicate.
A man with a strong family history of prostate cancer, a raised PSA, previous abnormal prostate tests, urinary symptoms, or known prostate disease should speak with a doctor before starting finasteride. The same applies to men already under urology follow up.
Finasteride may still be appropriate for some men, but PSA interpretation and prostate monitoring need to be handled properly. Starting finasteride without telling a doctor can make future prostate assessment harder.
When to speak with a doctor before using finasteride
Medical advice is especially important if you have:
- A raised or changing PSA result.
- A family history of prostate cancer, especially in a father or brother.
- Previous prostate biopsy or abnormal prostate examination.
- Urinary symptoms such as weak flow, frequent night urination, blood in urine, or difficulty starting urination.
- Current or past prostate cancer.
- New breast tenderness, breast swelling, nipple discharge, testicular pain, sexual side effects, mood changes, or depressive symptoms while using finasteride.
These symptoms do not automatically mean cancer, but they deserve proper assessment.
The practical conclusion
The long term prostate cancer studies do not show a simple harm signal that finasteride clearly increases prostate cancer deaths. The best known trial found fewer prostate cancer diagnoses overall, mainly fewer lower grade cancers. It also found more high grade cancers at diagnosis, but later analysis suggested this may have been partly due to better detection in smaller prostates. Long term survival was similar between the finasteride and placebo groups.
For hair loss patients, the main takeaway is practical rather than dramatic.
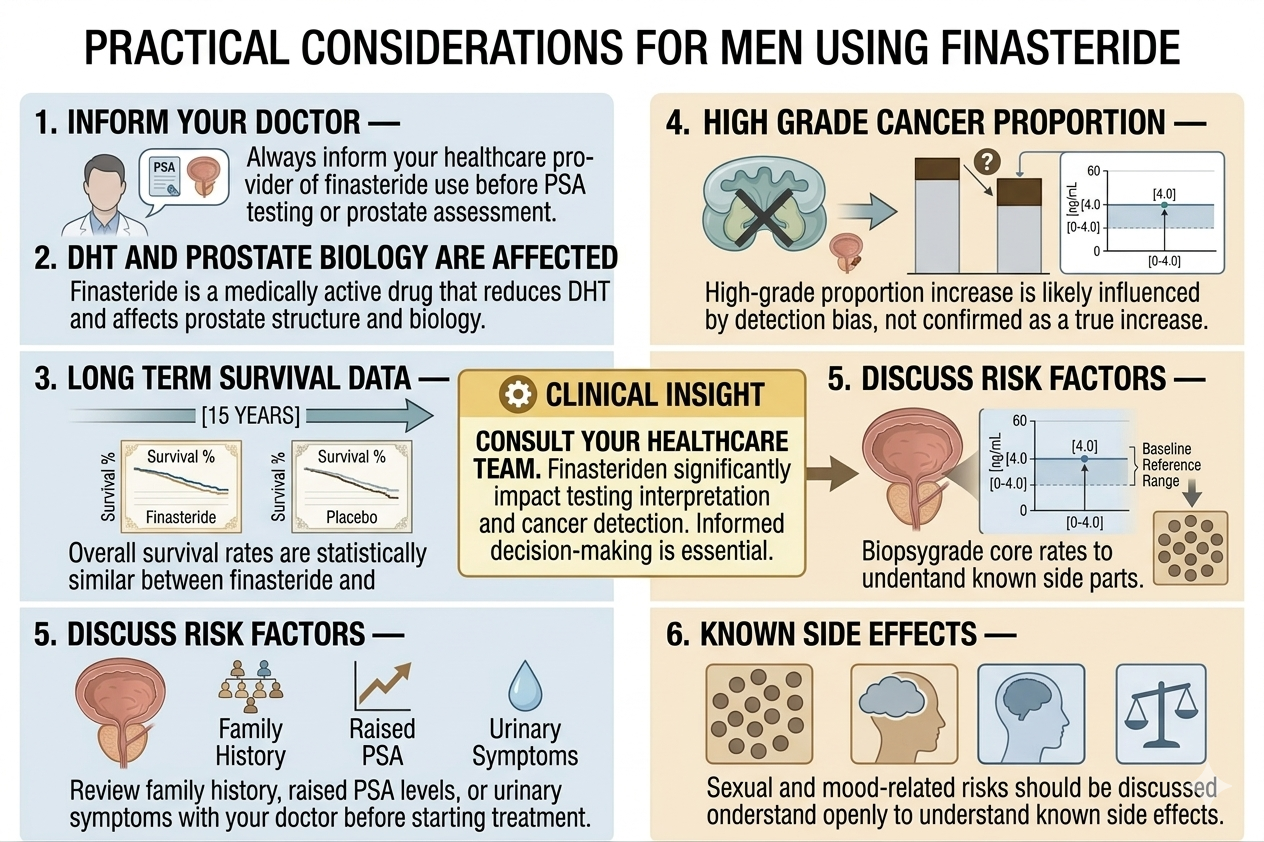
Finasteride is a medically active drug. It affects DHT, prostate size, and PSA interpretation. Men using it for hair loss should tell their doctor before PSA testing or prostate assessment. They should not use finasteride as a do it yourself prostate cancer prevention strategy. And they should weigh the potential hair benefits against known side effects, including sexual and mood related risks.
Used carefully, with proper medical awareness, finasteride remains an evidence based option for male pattern hair loss. But it should be treated as a real medicine, not as a cosmetic supplement.
Author: Dr. Priya Goswami
Medical review: Dr. Denis Broun
Next step
If you notice coverage changes without increased shedding, confirm what process is occurring.
Take the Hair Assessment to have a physician review your pattern, identify whether miniaturization is present, and determine appropriate staging and next steps.


Add Comment