Hair loss does not occur randomly across the scalp. In most men with androgen-related hair loss, thinning follows a recognisable pattern. Over time, the hairline may recede at the temples, the crown may become thinner, or both changes may occur together.
Doctors use classification systems to describe these patterns in a consistent way. The most widely used system for male pattern hair loss is the Norwood scale.
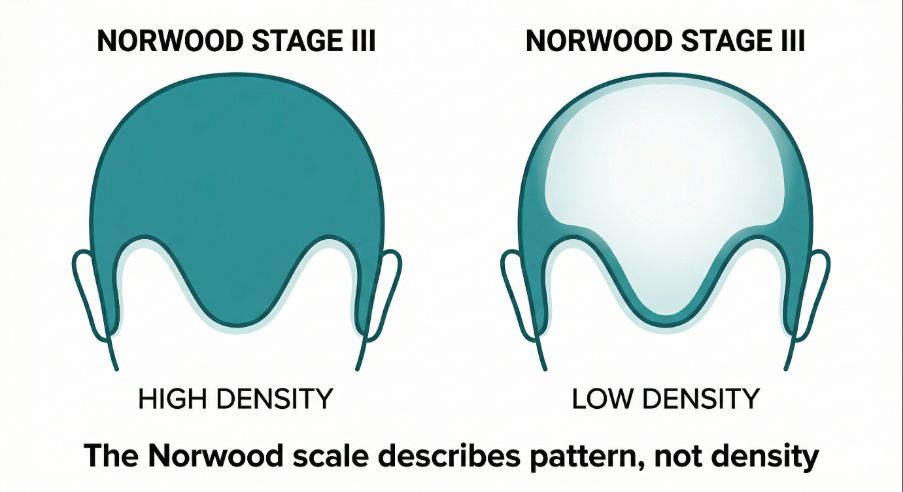
The Norwood scale does not measure how much hair someone has. Instead, it describes the pattern in which hair loss progresses across the scalp.
Understanding this distinction is important. The scale is a descriptive tool, not a diagnosis and not a measure of treatment success.
Understanding the hair growth cycle
To understand why classification systems exist, it helps to first understand how hair normally grows.
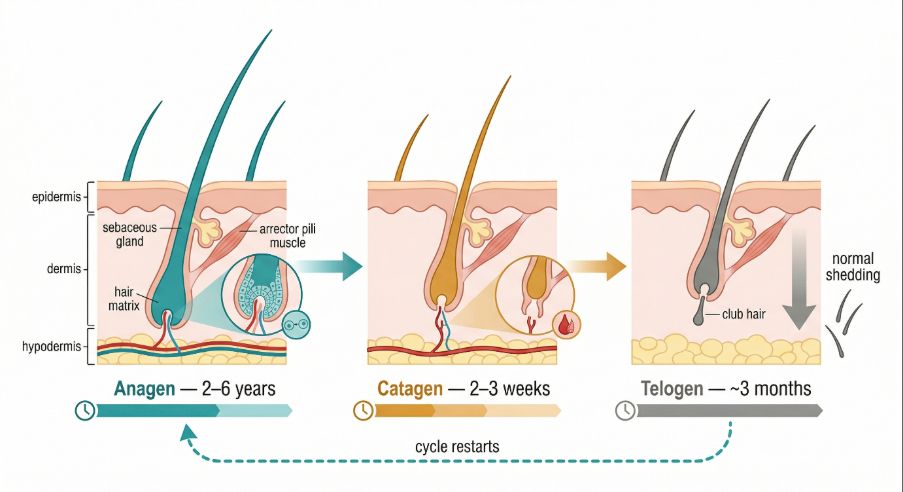
Each hair follicle on the scalp produces hair in a repeating cycle with three main phases.
- Anagen phase (growth phase)
During this phase the follicle actively produces a hair shaft. On the scalp this phase may last several years. - Catagen phase (transition phase)
The follicle gradually slows production and detaches from the hair shaft. - Telogen phase (resting phase)
Hair remains in place while the follicle prepares to begin a new growth cycle.
At any moment, different follicles on the scalp are in different phases of this cycle.
In some individuals, certain follicles are genetically sensitive to hormones known as androgens. When this sensitivity exists, repeated exposure to these hormones can gradually shorten the growth phase of affected follicles. The result is progressive thinning of hair shafts over time.
This process is called androgenetic alopecia, the most common cause of hair loss in men.
Why doctors classify hair loss patterns
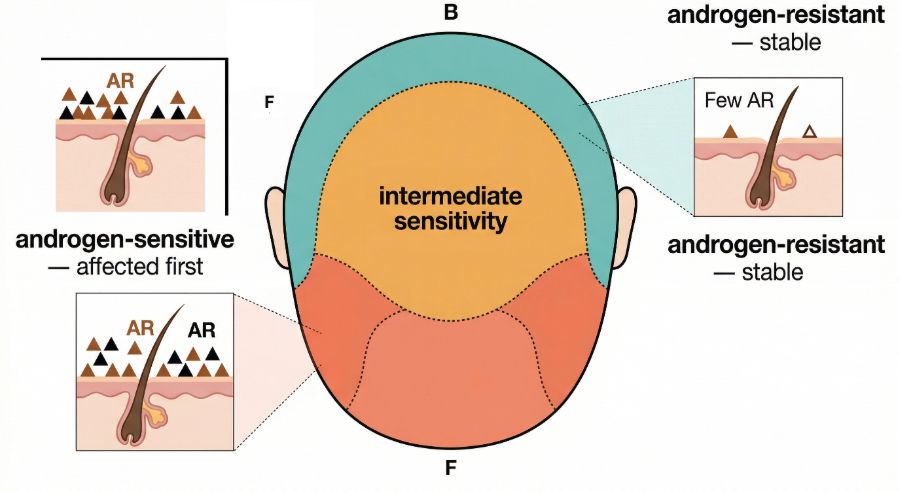
Hair thinning does not occur evenly across the scalp in androgenetic alopecia.
Certain regions are more sensitive to androgen signalling, particularly:
- the temples
- the frontal hairline
- the crown (vertex)
Other areas, especially the sides and back of the scalp, are usually less sensitive.
Because these differences create recognisable patterns of hair loss, clinicians developed staging systems to describe them. These systems allow doctors to:
- communicate clearly about the pattern of hair loss
- document how hair loss changes over time
- compare patterns between individuals
The Norwood scale is the most widely used of these staging systems.
What the Norwood scale measures
The Norwood scale describes the visible pattern of hair loss across the scalp.
It does not measure:
- the number of hairs on the scalp
- hair density
- the thickness of individual hairs
Two people classified at the same stage may have very different hair density.
The scale focuses mainly on two regions:
- the temporal hairline
- the crown (vertex)
Changes in these areas tend to follow a gradual progression that can be grouped into stages.
The stages of the Norwood scale
The Norwood scale typically includes seven main stages. Each stage describes a different pattern of hair loss progression.
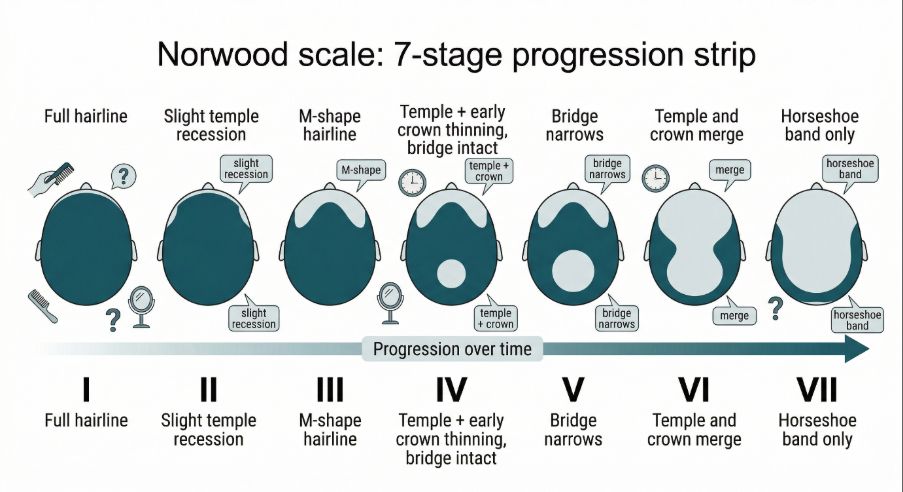
Stage I
Hair growth appears normal.
There is little or no visible recession of the hairline.
This stage does not necessarily indicate hair loss. Many individuals remain at this stage throughout life.
Stage II
The hairline begins to recede slightly at the temples.
This early recession may appear as a small triangular indentation on each side of the forehead. In many individuals this stage represents the beginning of androgen-related hairline changes.
Stage III
The recession at the temples becomes deeper and more clearly defined.
At this stage the frontal hairline typically forms a more noticeable “M” shape.
Stage III is often considered the earliest stage at which male pattern hair loss becomes clearly identifiable.
Stage III vertex
In some individuals, thinning first becomes visible at the crown rather than the temples.
This variant stage describes early thinning in the crown region while the frontal hairline remains relatively preserved.
Stage IV
Hairline recession becomes more pronounced.
At the same time, thinning at the crown becomes more visible. The frontal and crown areas are usually separated by a band of hair across the middle of the scalp.
Stage V
The thinning areas at the crown and the frontal scalp become larger.
The band of hair between them becomes narrower.
Stage VI
The frontal and crown thinning areas merge.
Hair remains mainly along the sides and back of the scalp.
Stage VII
This represents the most advanced stage of the pattern.
Hair is present mainly around the sides and back of the head. The top of the scalp has little remaining hair.
How clinicians use the Norwood scale
In clinical practice, the Norwood scale is primarily a descriptive tool.
Doctors may use it to:
- document the stage of hair loss during consultation
- monitor progression over time
- plan possible treatment approaches
- evaluate suitability for certain procedures
For example, some surgical hair restoration techniques require stable donor hair from the back of the scalp. Classification systems help doctors estimate how patterns of hair loss may evolve.
However, staging alone does not determine treatment decisions. Other factors are usually considered, including:
- age
- rate of hair loss progression
- family history
- hair density in donor areas
What the Norwood scale does not show
Although widely used, the Norwood scale has several limitations.
- First, it focuses mainly on pattern rather than density. Some individuals classified at an early stage may still experience significant thinning.
- Second, the scale was originally developed to describe typical male pattern hair loss. It does not capture all possible variations.
For example, some individuals experience diffuse thinning across the scalp rather than the classic pattern described in the Norwood stages.
- Third, the scale does not measure the biological processes occurring within follicles. It only describes visible changes.
Because of these limitations, doctors usually combine visual staging with other forms of examination.
Other ways hair loss may be evaluated
In addition to visual classification, clinicians may use several methods to evaluate hair loss.
These may include:
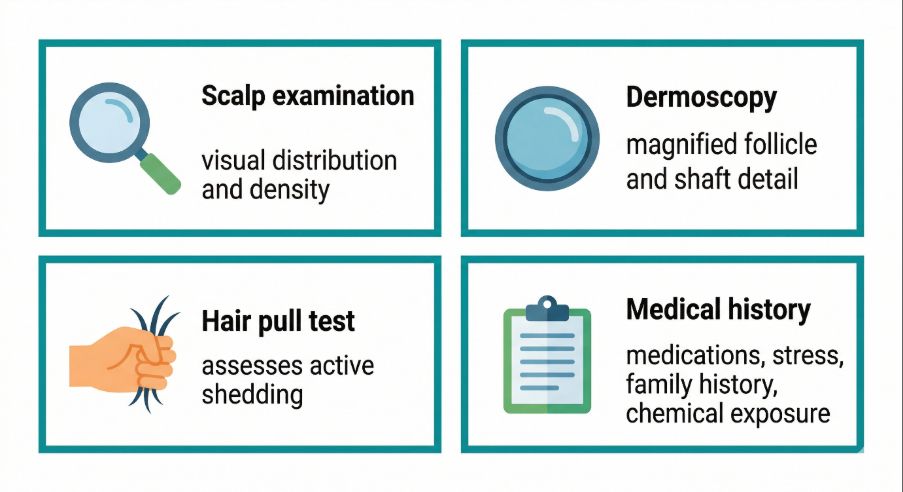
- Scalp examination
Visual assessment of hair distribution, density and scalp condition. - Dermoscopy
Magnified examination of hair shafts and follicles using specialised instruments. - Hair pull test
A simple method used to assess active shedding. - Medical history
Information about family history, medications, stress or illness may help identify contributing factors.
Together, these approaches help determine the underlying cause of hair thinning.
This review should include enquiry into exposure to medications known to affect the hair cycle — including anticoagulants, antihypertensives, retinoids, hormonal treatments, and oncology drugs — as well as occupational or environmental chemical exposures, which are recognised contributors to hair cycle disruption.
What research suggests about progression
Research suggests that androgenetic alopecia develops gradually over many years.
The rate of progression varies widely between individuals.
Some people may remain at an early Norwood stage for decades. Others may experience more rapid progression.
Genetic factors appear to play an important role. Studies have identified multiple genes associated with androgen sensitivity in scalp follicles.
Hormonal signalling, follicle miniaturisation and local scalp biology all contribute to the progression of hair thinning.
However, the precise mechanisms involved are still being studied.
Why understanding staging can be helpful
For individuals experiencing hair thinning, classification systems can provide a clearer picture of what is happening.
The Norwood scale offers a simple way to visualise how hair loss patterns may evolve.
At the same time, it is important to remember that staging systems are descriptive tools. They do not predict exactly how hair loss will progress in any one person.
Hair loss patterns can vary, and early evaluation by a qualified professional may help identify the underlying cause.
A practical perspective
Hair loss is a common experience, particularly with increasing age.
Classification systems such as the Norwood scale help clinicians describe patterns of hair thinning and track changes over time. They provide a shared language for discussing hair loss.
However, the scale does not measure the health of hair follicles, and it does not explain why hair loss occurs.
Understanding the biological processes behind hair growth and hair thinning remains an active area of dermatological research.
For individuals concerned about progressive hair loss, evaluation by a qualified dermatologist can help clarify the underlying cause and possible management options.
Author: Dr. Priya Goswami
Medical review: Dr. Denis Broun
Next step
If you notice coverage changes without increased shedding, confirm what process is occurring.
Take the Hair Assessment to have a physician review your pattern, identify whether miniaturization is present, and determine appropriate staging and next steps.
Add Comment