Hair loss is often associated with visible shedding -hair on the pillow, in the shower, or in the brush. For this reason, many people assume that if they are not shedding more than usual, hair loss cannot be occurring.
Clinically, this assumption is incorrect.
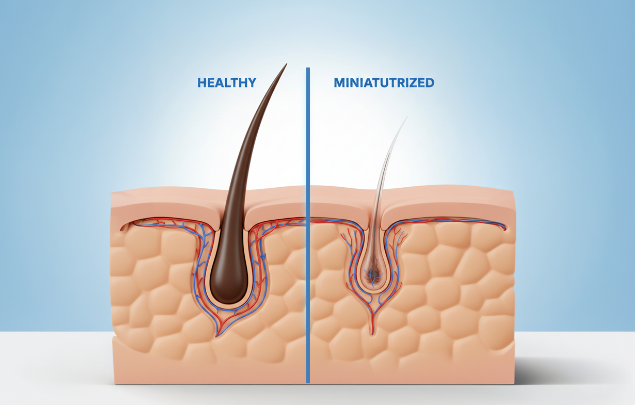
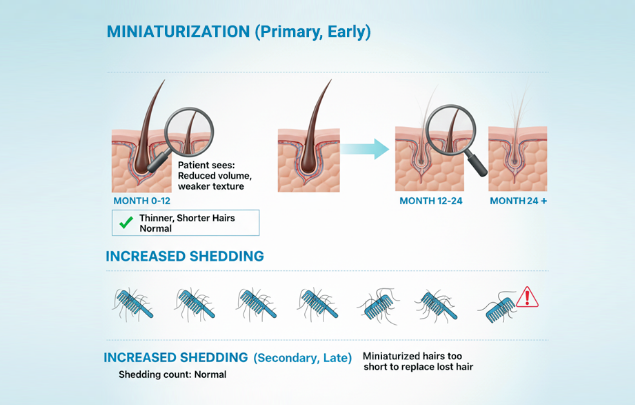
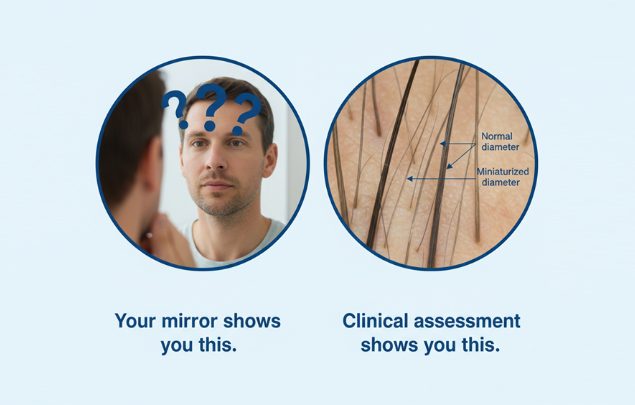
In early androgenetic alopecia, hair fall typically remains within normal daily ranges. The condition announces itself through diminishing hair quality, not increased hair quantity lost. The process does not begin with hairs being lost. It begins with follicle miniaturization -a progressive reduction in the diameter of individual hairs produced by genetically susceptible follicles.
Key distinction: Shedding describes how many hairs leave the scalp. Miniaturization describes the quality of hairs being produced. These are separate processes. In early patterned hair loss, miniaturization precedes increased shedding by months or years.
This pattern appears in both early frontal/temporal thinning and early central/part-line thinning. In both cases, the underlying process affects hair structure before it affects hair count. Hair may feel weaker, flatter, or more difficult to style long before any increase in shedding draws attention.
What Patients Usually Mean by "I'm Not Shedding"
When patients say they are "not shedding," they typically mean they see little hair on the pillow, in the shower drain, or in the brush. This observation is accurate regarding shedding itself, but it does not assess hair production.
From a clinical standpoint:
- Shedding = the exit of hairs from the scalp (increased in telogen effluvium, acute illness, postpartum states)
- Miniaturization = progressive reduction in hair shaft diameter (the defining feature of androgenetic alopecia)
- Thinning = the visible result of miniaturization (reduced coverage despite stable hair count)
These are separate processes. Androgenetic alopecia is primarily a miniaturization disorder, not a shedding disorder.
What patients notice when miniaturization is present but shedding is unchanged:
- Hair feels finer or less resilient
- Styles lose volume more quickly
- Hairline looks less defined, or part appears wider
- Hair appears flatter despite similar length
In early androgenetic alopecia, the hair cycle continues normally. Hairs grow, rest, and shed within expected ranges. What changes is the output of each follicle. Over successive cycles, individual hairs emerge thinner, shorter, and less pigmented. Because daily shed counts remain stable, this process progresses silently.
Important: Shedding reflects hair exit. Miniaturization reflects follicle output. In early androgenetic alopecia, output is affected before exit increases.
If texture or coverage changes persist despite stable shedding, shedding counts cannot provide accurate diagnostic context.
How Miniaturization Progresses Without Increased Shedding
Early androgenetic alopecia is driven by follicle miniaturization, not by sudden or excessive shedding. This is why the condition progresses even when hair fall appears normal.
The mechanism
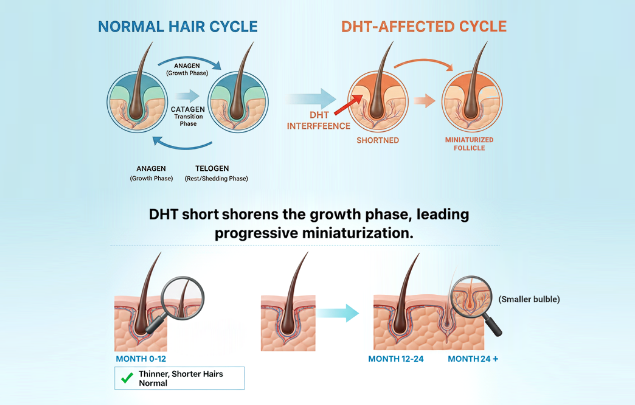
Each follicle follows a growth cycle: produce hair, rest, shed, repeat. In androgenetic alopecia, this cycle remains intact. What changes is the product.
With each cycle, affected follicles produce hairs that are:
- Thinner in diameter
- Shorter in length
- Less structurally robust
Because follicles continue cycling, shedding does not initially increase.
What this looks like clinically:
- Reduced density without obvious hair fall
- Decreased volume, especially under certain lighting
- Less defined hairlines or part lines
- More difficult styling despite stable shedding
These changes reflect reduced hair quality and coverage, not reduced hair count.
The hormonal driver
Follicle miniaturization is driven by androgen sensitivity. In genetically susceptible follicles, dihydrotestosterone (DHT) progressively:
- Shortens the growth phase
- Reduces hair shaft diameter
- Limits the cosmetic contribution of each hair
Because this process is gradual, clinical changes remain subtle for extended periods.
Why shedding is a late sign
As long as follicles cycle, hair fall may appear normal. Noticeable shedding typically occurs only after miniaturization is well-established and follicles begin producing hair too short to replace shed hairs. By this stage, the process is no longer early.
The absence of increased shedding does not exclude active androgenetic alopecia. It indicates the process is occurring at the level of follicle output, not follicle loss.
How the Same Process Produces Different Patterns
Follicle miniaturization follows consistent biological mechanisms, but visible patterns vary based on which follicles are genetically susceptible.
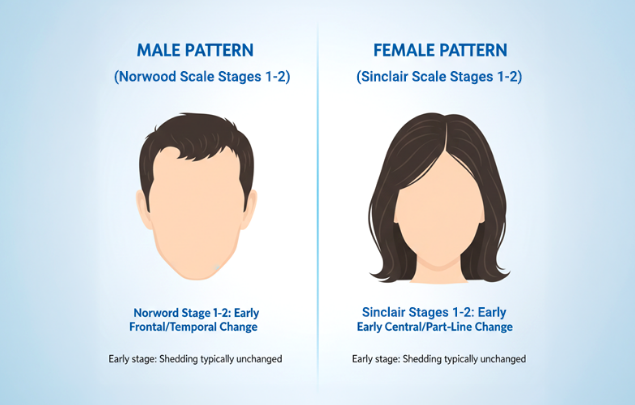
Early frontal and temporal change (male pattern)
In individuals with frontal/temporal susceptibility, miniaturization typically begins along the hairline and temples. This pattern is staged using the Norwood scale (male androgenetic alopecia).
Early stages (Norwood 1–2):
- Hairline appears less defined rather than clearly receded
- Temple density softens before shape changes
- Shedding remains normal
Early central and part-line change (female pattern)
In individuals with central scalp susceptibility, miniaturization often presents as gradual thinning along the midline. This pattern is staged using the Sinclair scale (female androgenetic alopecia).
Early stages (Sinclair 1–2):
- Central part appears slightly wider
- Density reduced under overhead lighting
- Hair fall remains unchanged
Important: The Norwood and Sinclair scales describe sex-specific patterns of the same condition - androgenetic alopecia. At early stages, both reflect follicle miniaturization without increased shedding.
Why early patterns are missed
Because follicles remain active:
- Hair continues growing
- Shedding stays within normal limits
- Changes develop gradually
Many patients do not recognize early androgenetic alopecia until the pattern becomes visually obvious.
Clinical implication
Different visible patterns do not indicate different diseases. Both patterns involve progressive follicle miniaturization driven by androgen sensitivity. Early evaluation focuses on pattern, stage, and progression risk - not on waiting for shedding to appear.
Why Visual Self-Monitoring Misses Early Miniaturization
Patients often rely on mirrors, daily observation, or shedding counts to assess hair changes. In early miniaturization, these methods are unreliable — not because changes are insignificant, but because they are gradual, structural, and comparative.
Daily observation hides gradual change
Miniaturization develops over months to years. When viewed daily, the brain adapts to small shifts, making progression difficult to recognize. This applies to both Norwood-type and Sinclair-type early changes.
Shedding counts are poor proxies
Because follicles cycle normally in early stages:
- Daily shed counts remain stable
- Hair fall fluctuates for unrelated reasons (season, stress, illness)
- Shedding does not reflect hair shaft diameter
Stable shedding coexists with active miniaturization.
External variables distort perception
Coverage perception varies with:
- Overhead or directional lighting
- Hair length and weight
- Styling habits or product use
These mask or exaggerate early changes, making casual assessment unreliable.
What structured comparison reveals
Without consistent reference points, these changes go unnoticed:
- Gradual reduction in hair shaft calibre
- Progressive softening of hairline definition
- Slow widening of central part
Subtle structural change is easier to detect retrospectively than in real time.
Clinical assessment criteria
Evaluation does not rely on single observations. It assesses:
- Patterned distribution consistent with androgenetic alopecia
- Evidence of miniaturization (reduced shaft diameter)
- Change over time or clear signs of pattern hair loss
This determines whether miniaturization is stable, slowly progressive, or inactive — regardless of shedding patterns.
What Diagnosis-Led Evaluation Clarifies
In androgenetic alopecia, the clinical question is not whether shedding is present, but whether follicles are producing progressively smaller hairs.
Assessment components
Clinical evaluation examines features unreliable to self-assess:
| Feature | What It Indicates |
|---|---|
| Hair shaft diameter variation | Miniaturization activity within a region |
| Pattern distribution | Norwood-type, Sinclair-type, or overlap |
| Relative stage | Focal, diffuse, or progressing across zones |
These features determine whether miniaturization is present and active, independent of shedding.
Why clinical evaluation detects what self-assessment cannot
Miniaturization begins with progressive changes in follicle output, not increased hair fall. Microscopically, susceptible follicles produce hairs of uneven and gradually reducing diameter across cycles. This variability is not detectable through mirrors or shedding awareness.
Research demonstrates that DHT alters follicle signaling by shortening growth phase and reducing shaft calibre before shedding increases or follicles are lost. Hair loss may be active when visible density appears stable and hair fall seems unchanged.
Structured evaluation captures:
- Variation in hair shaft diameter within regions
- Patterned distribution consistent with early Norwood or Sinclair stages
- Evidence of progressive miniaturization vs. stable variation
Without this assessment, early androgenetic alopecia is commonly underestimated. With it, follicle status can be defined accurately, progression risk assessed, and next steps considered in correct biological context.
What this enables
Once miniaturization pattern and stage are defined:
- Progression risk discussed realistically
- Monitoring becomes intentional rather than reactive
- Treatment options considered in correct context
The value is mechanism clarity, not reassurance or assumption.
When Structured Evaluation Becomes Relevant
When miniaturization is the suspected process, the question is not whether shedding is present, but whether follicle output has changed in a patterned way.
At early stages, this change is subtle. Hair grows. Shedding remains normal. What shifts is the consistency, calibre, and coverage contribution of individual hairs. These changes cannot be reliably confirmed through casual observation.

Evaluation is indicated when:
- Hair texture, volume, or coverage changes despite stable shedding
- Frontal, temporal, or central pattern emerges
- Uncertainty exists about whether changes are stable or progressive
Evaluation does not commit to treatment. It establishes baseline: whether miniaturization is present, where it is occurring, and how advanced it appears.
This clarity enables intentional monitoring and ensures future decisions rest on follicle status and stage, not assumption.
Next step
If you notice coverage changes without increased shedding, confirm what process is occurring.
Take the Hair Assessment to have a physician review your pattern, identify whether miniaturization is present, and determine appropriate staging and next steps.

Add Comment